
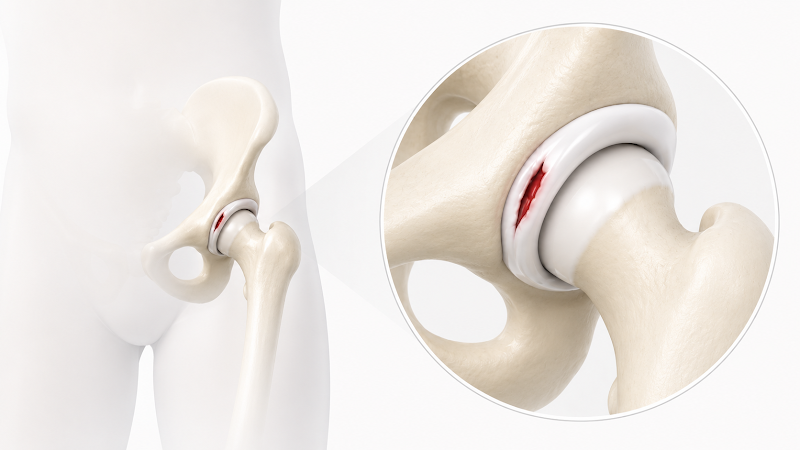
Hip labrum tears are very common among athletes in sports that involve quick pivoting, deep hip flexion, repetitive stress or high-impact collisions; we see them most often in soccer and hockey players, gymnasts and runners. Symptoms include pain in the groin, buttocks or side of the hip that can be sharp or dull, a clicking or locking sensation or the feeling that the hip is giving way during movement, or general stiffness in the hip. Chronic hip flexor strains are also a telltale sign of a labrum tear, as referred pain from the labrum often presents as a recurrent groin strain.
Over the past 10 years, we at Academy Orthopedics have been privileged to contribute to meaningful advancements in hip arthroscopy for the treatment of labral tears, femoroacetabular impingement and dysplasia. As shown in our studies below, innovations such as labral augmentation, the pericapsular nerve group (PENG) block and the postless surgical table have led to improved surgical outcomes across patient populations.
What is Femoroacetabular Impingement (FAI)?
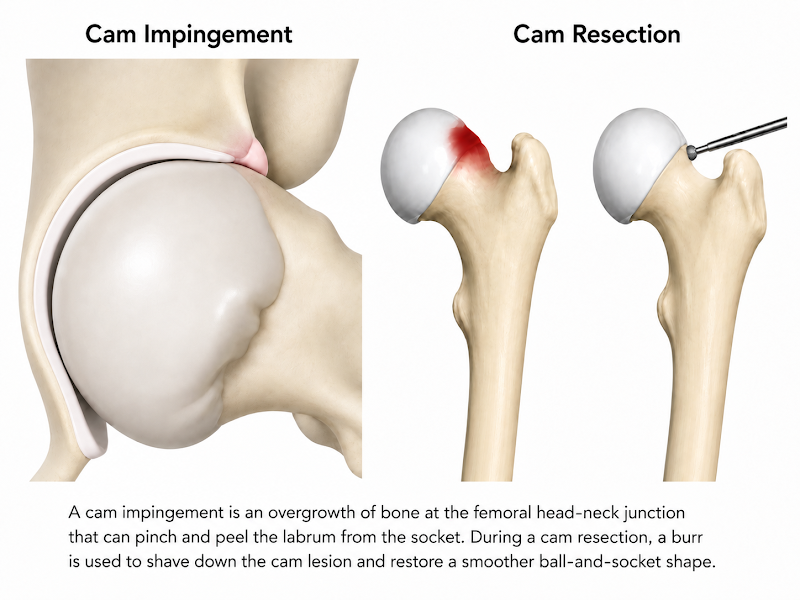
Femoroacetabular impingement, or FAI, occurs when the ball-and-socket bones of your hip joint are abnormally shaped. Because they do not fit together perfectly, the bones rub and pinch against each other during movement, leading to pain and cartilage or labral damage. This damage often occurs during adolescence when you’re growing and developing and playing a lot of sports; you’ll often put a lot of stress on the front of the growth plate from squatting and cutting and pushing off, and you will develop a bump on the ball part of the ball-and-socket. That bump rubs against the edge of the socket and can damage the labrum, which acts as a gasket around the ball-and-socket. We call this “athlete’s hip.” Though this damage begins in adolescence, you may not actually feel pain until you’re in your 20s or 30s or 40s.
What is Hip Dysplasia?
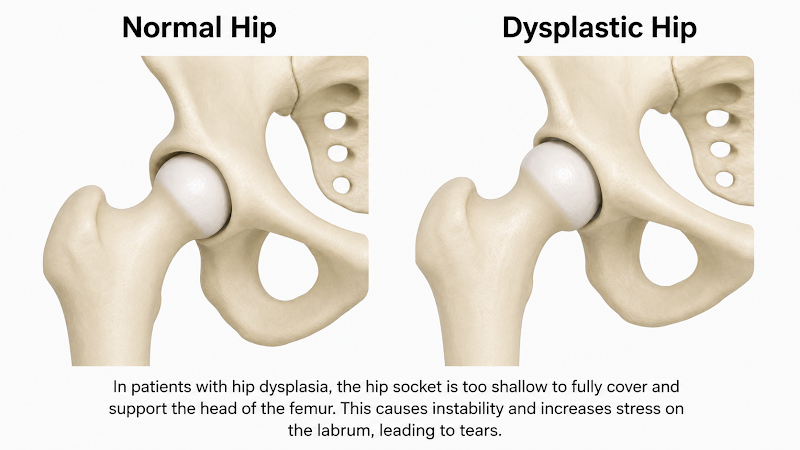
Hip dysplasia is a condition in which the hip socket is too shallow to fully cover and support the head of the femur. This structural deficiency leads to instability, pain and an increased risk of early arthritis. It is also a leading cause of labral tears, as the labrum – the ring of cartilage that acts like a gasket or washer to stabilize the joint – is forced to overcompensate for the lack of bone support.
Labral Repair Versus Labral Augmentation
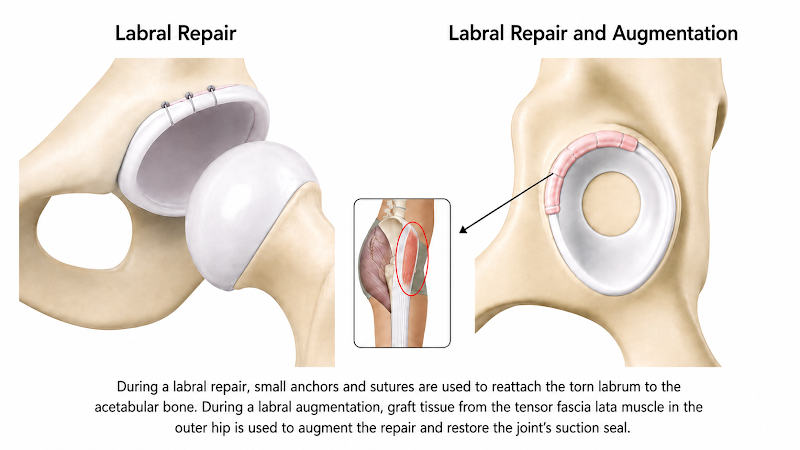
In the past, many patients with borderline hip dysplasia required a periacetabular osteotomy (PAO), during which the bone around the hip socket is reshaped or realigned to correct deformities or improve coverage or alignment. Today, however, we are increasingly able to treat patients with borderline dysplasia or ligament laxity, including those with Ehlers-Danlos syndromes, with labral augmentation to improve stability rather than traditional labral repair with a subsequent PAO. Our study, published in Arthroscopy, Sports Medicine, and Rehabilitation in August of 2025 confirmed these successful patient outcomes.
During labral augmentation, we use donated tissue to rebuild the labrum to increase the stability of the hip joint, as opposed to only repairing the patient’s native tissue. This donated cadaver tissue is an allograft from the tensor fascia lata (TFL) muscle on the outer thigh. Whether the patient’s own tissue has been shredded over the years and is no longer of good quality, or there is less bony coverage or a laxity in the hip, we can now augment our repairs with this TFL allograft to make the labrum more stable. Over time, the allograft integrates with the patient’s own labral tissue, creating a larger, more stable labrum than the patient had even before the labrum was damaged. This advancement has given patients who would not have done as well with hip arthroscopy in the past a less-invasive surgical option.
The Pericapsular Nerve Group (PENG) Block
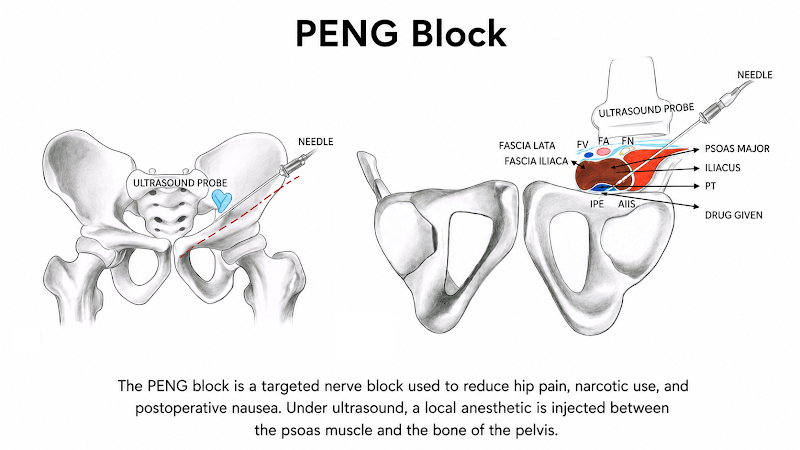
There are a variety of nerve blocks that can be used to decrease post-operative pain and the need for narcotic pain relievers during and after shoulder and knee surgery, but until recently, we did not have a similar option for the hip. However, the PENG block, an ultrasound-guided injection of local anesthetic used to block the sensory nerves supplying the hip capsule, has provided a great option for hip arthroscopy.
Our research, published in Arthroscopy: The Journal of Arthroscopic and Related Surgery in February 2023, has demonstrated that the PENG block improves pain throughout the patient’s surgical experience. Patients require fewer narcotic and anti-nausea medications while maintaining motor function, which allows for earlier and more effective rehabilitation.
Reducing narcotic use is incredibly important, especially in younger patients. The PENG block results in decreased pain immediately after surgery, which often prevents a prolonged cycle of pain and dependency on pain medications. Patients who experience better early pain control are more likely to engage in effective rehabilitation and achieve improved long-term outcomes.
Postless Hip Arthroscopy
Traditionally, a perineal post – a padded structure placed in the groin area – has been used during hip arthroscopy to provide countertraction while the operative leg is pulled to create space within the joint. However, this technique can compress the nerves and soft tissues in the groin, often resulting in “accepted” side-effects, such as numbness, bruising, skin tears or pain.
To address this problem, we at Academy Orthopedics did research on a postless surgical bed topped with a grippy, sponge-like pad. This innovation allows surgeons to achieve controlled traction without the need for a perineal post.
The result is more precise, incremental joint distraction and a significant reduction in post-operative complications. Our research, published in Arthroscopy in 2025, demonstrated that patients undergoing hip arthroscopy with the postless hip distraction system experienced significantly improved patient-reported outcomes and fewer post-surgical side effects when compared with conventional post-assisted hip arthroscopy patients at the one-year mark.
Dr. Anthony Scillia is a surgical specialist in shoulder, elbow, hip and knee arthroscopy and joint preservation.


